


{kind=link}
{kind=link}
{kind=link}
Hubsiino Healthcare Consulting © 2020. All Rights Reserved.

What is Blood Pressure?
Blood pressure(BP) is the most important of vital signs (BP, heart rate, temperature and respiratory rate). After your age, gender and smoking history, your BP is the best indication of how long you will live and what percentage of your life you will spend disabled by the damage done to your body by an “unhealthy BP”: Stroke, heart failure, kidney failure, heart attack and hardening of the arteries called atherosclerosis. This is like rust in old pipes. When the rust gets too bad the blood flow cannot get to where it needs to be.
What is Blood Pressure itself?
Blood pressure (BP) is the force of the blood against artery walls when the heart contracts and pumps blood into the circulatory system; this is called systolic pressure. When the heart relaxes between beats, the BP decreases and is called diastolic pressure. Blood pressure is determined by the amount of blood the heart pumps [cardiac output CO= Stroke volume x heart rate) and the amount of resistance to blood flow in the arteries. BP= CO x resistance to flow.
Blood pressure is measured in millimeters of mercury (mm Hg) and recorded with the systolic number first, followed by the diastolic number. For example, a normal blood pressure would be recorded as something under 120/80 mm Hg.
How was BP first measured? Reverend Stephen Hales (UK)was the first person to measure arterial pressure, as direct intra-arterial pressure in the horse in 1733.
Direct intra-arterial pressure measurement in the horse.
Almost a century later, sphygmographic devices were developed to measure blood pressure noninvasively in humans. The early devices were cumbersome and relatively insensitive. The introduction of the sphygmomanometer into clinical medicine in the late 1800s and early 1900s was accepted by some practitioners as a valuable aid to diagnosis. After Korotkoff’s 1905 landmark description of the sounds associated with the appearance of the pulse wave, there was little change in the measurement of blood pressure in the first half of the 20th century. Towards the end of the 20th century, due to primarily on mercury-related health concerns, the mercury manometer has essentially been replaced with aneroid and electronic devices, but it is still used for calibrating these devices, and standardized protocols have been recommended to assure their accuracy.
Mercury Sphygmanometer BP monitor Aneroid arm BP Monitor Automatic Arm BP Monitor
As techniques for measuring blood pressure improved and increasing evidence for a blood pressure-mortality relationship became apparent, more companies began to require blood pressure measurements of insurance applicants. By1918, companies were measuring systolic and diastolic blood pressure by auscultation, under somewhat standardized conditions, rather than simply systolic blood pressure by palpation. In a series of reports between 1925 and 1979, the Actuarial Society of America described the population-based distribution of blood pressure, the age-related increases of blood pressure, and the relationships of blood pressure to both body size and cardiovascular morbidity and mortality (Framingham study 1948). However, the discovery of drugs in the 1950s that lowered BP, led to the implementation of large-scale trials in the 1960s (Veterans Administration Cooperative Studies of Hypertension) and early 1970s (Hypertension Detection and Follow-up Program (HDFP), which demonstrated that reduction in morbidity and mortality from hypertension patients could be attained by treating, and the risks of lowering this unhealthy BP outweighed the risks of not lowering. Because patients whose BP rises to unhealthy levels usually have no symptoms to suggest the presence of this condition, the only way to detect the “silent killer” is to measure the BP accurately. Thus, the major reason for measuring BP in the office is to detect the evolution of an unhealthy BP, which is that level of blood pressure (140/90 mmHg) above which you (or your patient) are healthier in the long run if that BP is lowered; this was suspected by observational studies and proven by clinical trials. Most trials have been based on human measurements and a mercury manometer and AHA guidelines.
Careful Blood Pressure Measurement is very important for the health care system, and it is the most important skill you will learn in your medical career. Do it correctly and you will help more patients to better health than with any other skill you learn. Do it wrong and you will harm more patients than with any other medical errors you make over your career. “(CE Grim MD 1991: UCLA Preventive Medicine Curriculum, Blood Pressure Measurement Training and Certification Program, First year)”. Studies show that even a “small” (5 mm Hg) systematic BP measurement error can have an effect on the prevalence of hypertension in the population by erroneously classifying normotensives to hypertensives and vice versa in great numbers resulting in denial of treatment for those needed (HDFP study).
The recommended gold standard for office blood pressure measurements by the latest American Heart Association is:
a. The auscultatory method using a mercury manometer or aneroid. b. Any electronic device that has been validated as accurate by the American Association for the Advancement of Medical Instrumentation (AAMI3)?
A blood pressure reading has a top number (systolic) and bottom number (diastolic). Normal blood pressure is less than 120 over 80 (120/80). People whose blood pressure is above the normal range should ask their doctor how to lower it.
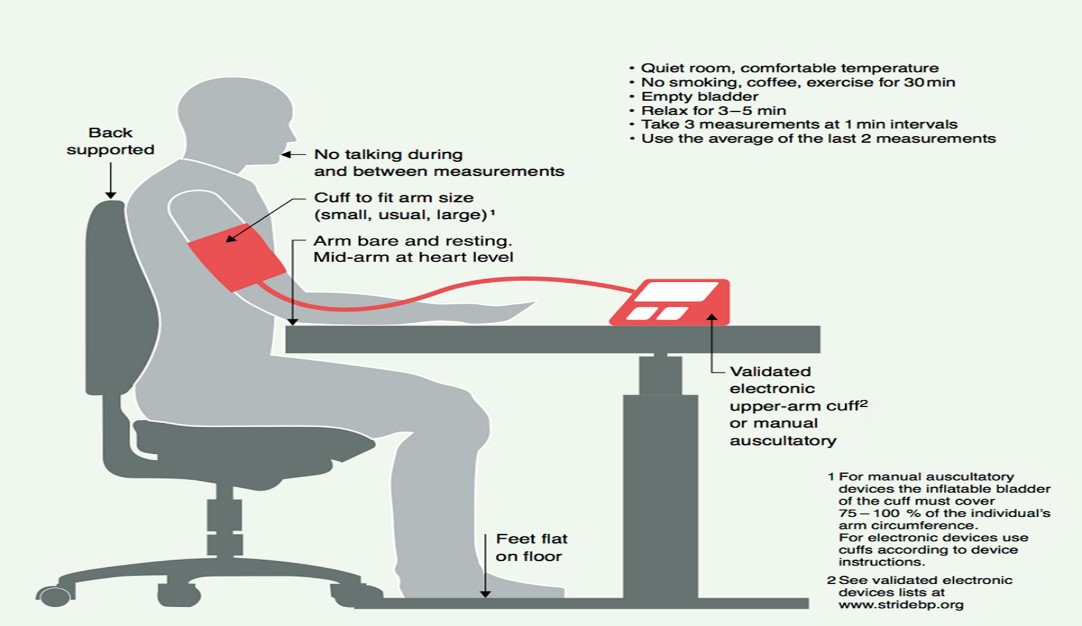
Correct measurement of blood pressure
Definition of Hypertension
Epidemiology of hypertension
Hypertension is the single most important preventable cause of premature death in developed countries. Sixty percent of adults’ office visit is related to hypertension. It is the leading cause of cardiovascular disease and premature death worldwide. The prevalence of this public health problem is increasing in low- and middle-income countries (LMICs) in both urban and rural communities. The global prevalence of hypertension was estimated to be 1.13 billion in 2015. Hypertension remains the leading cause of death globally, accounting for 10.4 million deaths per year. BP trends show a clear shift of the highest BPs from high-income (HIC) to low-income regions, with an estimated 349 million with hypertension in HIC and 1.04 billion in LMICs. The large disparities in the regional burden of hypertension are accompanied by low levels of awareness, treatment and control rates in LMIC, when compared to HIC. The highest prevalence is observed in blacks in the western hemisphere (the prevalence in African Americans (AA) is among the highest in the world, and in 2011 to 2014 was 45.0% and 46.3% among AA males and females, and are 30% more likely to die from CV diseases than whites) and central and eastern European countries. The overall prevalence of hypertension in adults is around 30 - 45%, with a global age standardized prevalence of 24 and 20% in men and women, respectively, in 2015. This high prevalence of hypertension is consistent across the world, irrespective of income status, i.e., in (LMIC) and higher income countries. Hypertension has become progressively more common with advancing age, with a prevalence of >60% in people aged >60 years. As populations age, adopt more sedentary lifestyles, and increase their body weight, the prevalence of hypertension worldwide will continue to rise. It has been estimated that the number of people with hypertension will increase by 15–20% by 2025, reaching close to 1.5 billion.
Causes of hypertension:
Older age, Obesity, Smoking, Low physical activity, and Khat chewing (a drug found in the leaves of a wild, East African shrub called Catha edulis. The plant contains a central nervous system stimulant called cathinone and is used in East Africa and Arabian Peninsula), Family history, sleep apnea, higher salt sensitivity, and stress. Eighteen genotypes and intermediate phenotypes were implicated with an increase of blood pressure by the research done by Kaplan &Victor et al.
Diagnostics:
Hypertension is also diagnosed in the following situations:
Source: National Health and Nutrition Examination Survey (NHANES)
Management of hypertension
Lifestyle changes
Healthy lifestyle choices can prevent or delay the onset of hypertension and can reduce Cardiovascular (CV) risk. Effective lifestyle changes may be sufficient to delay or prevent the need for drug therapy in patients with grade 1 hypertension. They can also intensify the effects of BP lowering therapy, but they should never delay the initiation of drug therapy in patients with end organ damage or at a high level of CV risk. A major disadvantage of lifestyle modification is the poor persistence over time. The recommended lifestyle measures that have been shown to reduce BP are:
Salt restriction, moderation of alcohol consumption, high consumption of vegetables and fruits, weight reduction and maintaining an ideal body weight, and regular physical activity. In addition, tobacco smoking has an acute prolonged pressor effect that may raise daytime ambulatory BP, but smoking cessation and other lifestyle measures are also important beyond BP (i.e., for CVD and cancer prevention). Moderation of alcohol consumption and cessation of Khat chewing in East Africa and Arabian Peninsula is also very important. Dietary sodium restriction: there is evidence of a causal relationship between sodium intake and BP, and excessive sodium consumption (>5 g sodium per day, e.g., one small teaspoon of salt per day) has been shown to have a pressor effect and be associated with an increased prevalence of hypertension and the rise in SBP with age. Conversely, sodium restriction has been shown to have a BP-lowering effect in many trials. A recent meta-analysis of these trials showed that a reduction of 1.75 g sodium per day (3.4 g salt/day) was associated with a mean 4.2/2.1 mmHg reduction in SBP/DBP, with a more pronounced effect (-5.4/ -2.8 mmHg) in people with hypertension. The beneficial effect of a reduced sodium intake on BP tends to diminish with time, in part due to poor dietary persistence. The BP-lowering effect of sodium restriction is greater in black people, in older patients, and in patients with diabetes, metabolic syndrome, or Chronic Kidney Disease. In people with treated hypertension, effective sodium restriction may reduce the number or dose of BP-lowering drugs that are necessary to control BP. The effect of reduced dietary sodium on CV events remains unclear. Prospective cohort studies have reported an overall increased risk of mortality and CV events on high sodium intake. However, they also reported that reducing sodium intake below a certain level (about 3 g of sodium per day) further reduced BP, but paradoxically was associated with an increased risk of all-cause and CV mortalities in both the general population and in hypertensive people, suggesting a J-curve phenomenon. Other dietary changes Hypertensive patients should be advised to eat a healthy balanced diet containing vegetables, legumes, fresh fruits, low-fat dairy products, wholegrains, fish, and unsaturated fatty acids (especially olive oil), and to have a low consumption of red meat and saturated fatty acids. Regular physical activity: Physical activity induces an acute rise in BP, especially SBP, followed by a short-lived decline in BP below baseline. Epidemiological studies suggest that regular aerobic physical activity may be beneficial for both the prevention and treatment of hypertension, and to lower CV risk and mortality.
Effective lifestyle changes may be sufficient to delay or prevent the need for drug therapy particularly in hypertensive patients from LMIC because of the scarcity and the cost of the drugs.
Drugs therapy
Most patients will require drug therapy in addition to lifestyle measures to achieve optimal BP control. There are ten (10) classes of hypertensive medication with Aliskiren (Renin antagonists) as the newest, which should be used carefully, because they stay in blood for one month and without renin there is a risk not to acknowledge dehydration and other volume depletions. However, in recent Guidelines, five major drug classes were recommended for the treatment of hypertension: ACEI (angiotensin-converting enzyme inhibitors), ARBs (angiotensin receptor blocker), beta-blockers, CCBs (calcium channel blocker), and diuretics (thiazides and thiazide-like diuretics such as chlortalidone and indapamide), based on: (a) proven ability to reduce BP; (b) evidence from placebo-controlled studies that they reduce CV events; and (c) evidence of broad equivalence on overall CV morbidity and mortality, with the conclusion that benefit from their use predominantly derives from BP lowering. These conclusions have since been confirmed by lifestyle interventions for patients with hypertension or high-normal. Other classes of drugs have been less widely studied in event-based RCTs or are known to be associated with a higher risk of adverse effects [e.g., alpha-blockers, centrally acting agents, and mineralocorticoid receptor antagonists (MRAs)]. These are useful additions to antihypertensive drugs in patients whose BP cannot be controlled by proven combinations of the aforementioned major drug classes.
Adherence to Antihypertensive Treatment
Background
Following a diet or executing lifestyle changes corresponds with agreed recommendations from a healthcare provider. Non-adherence to antihypertensive treatment affects 10%–80% of hypertensive patients and is one of the key drivers of suboptimal BP control. Poor adherence to antihypertensive treatment correlates with the magnitude of BP elevation and is an indicator of poor prognosis in hypertensive patients. The etiology of nonadherence to antihypertensive treatment is multifactorial and includes causes associated with the healthcare system, pharmacological therapy, the disease, patients and their socioeconomic status, and patients’ health literacy.
Recommendations: Adherence to Antihypertensive Therapy
Common and Other Comorbidities and Complications of Hypertension
Background
Common Comorbidities and Complications
Management of Comorbidities
Specific Circumstances
There are specific circumstances in hypertension management requiring thorough investigation and screening to identify the causes and institute appropriate targeted treatment.
Resistant Hypertension
Resistant hypertension is defined as seated office BP >140/90 mm Hg in a patient treated with three or more antihypertensive medications at optimal (or maximally tolerated) doses including a diuretic and after excluding pseudoresistance (poor BP measurement technique, white coat effect, nonadherence and suboptimal choices in antihypertensive therapy) as well as the substance/drug-induced hypertension and secondary hypertension.79 Resistant hypertension affects around 10% of hypertensive individuals, has a negative impact on well-being106 and increases the risk of coronary artery disease, chronic HF, stroke, end-stage renal disease, and all-cause mortality.107 Approximately 50% of patients diagnosed with resistant hypertension have pseudoresistance rather than true resistant hypertension.
Secondary Hypertension
A specific cause of secondary hypertension can be identified in 5%–10% of hypertensive patients. Early diagnosis of secondary hypertension and the institution of appropriate targeted treatment have the potential to cure hypertension in some patients or improve BP control/reduce the number of prescribed antihypertensive medications in others. The most common types of secondary hypertension in adults are renal parenchymal disease, renovascular hypertension, primary aldosteronism, chronic sleep apnea, and substance/drug-induced.
Hypertension in Pregnancy
Hypertension in pregnancy is a condition affecting 5%–10% of pregnancies worldwide. Maternal risks include placental abruption, stroke, multiple organ failure (liver, kidney), disseminated vascular coagulation. Fetal risks include intrauterine growth retardation, preterm birth, intrauterine death.
Leave your comment